What we know — and don't — about Zika, ten years on
Zika remains a WHO priority pathogen — it spreads via Aedes mosquitoes, can cross from mother to baby in pregnancy, and was responsible for the 2015–16 microcephaly emergency that prompted the WHO to declare a Public Health Emergency of International Concern in February 2016. Yet a decade on, the parameters that decide how Zika spreads, who it harms, and how to model the next outbreak remain scattered across hundreds of papers — often using inconsistent definitions.
A new systematic review and meta-analysis from Imperial's MRC Centre for Global Infectious Disease Analysis, co-led by Dr. Kelly McCain and Dr. Anna Vicco, with senior authors Dr. Ruth McCabe and Assoc. Prof. Ilaria Dorigatti brings this body of evidence into one place. The authors screened 27,491 studies, included 574, and curated 969 epidemiological parameters, 127 outbreak records, and 154 transmission models from across 59 countries.
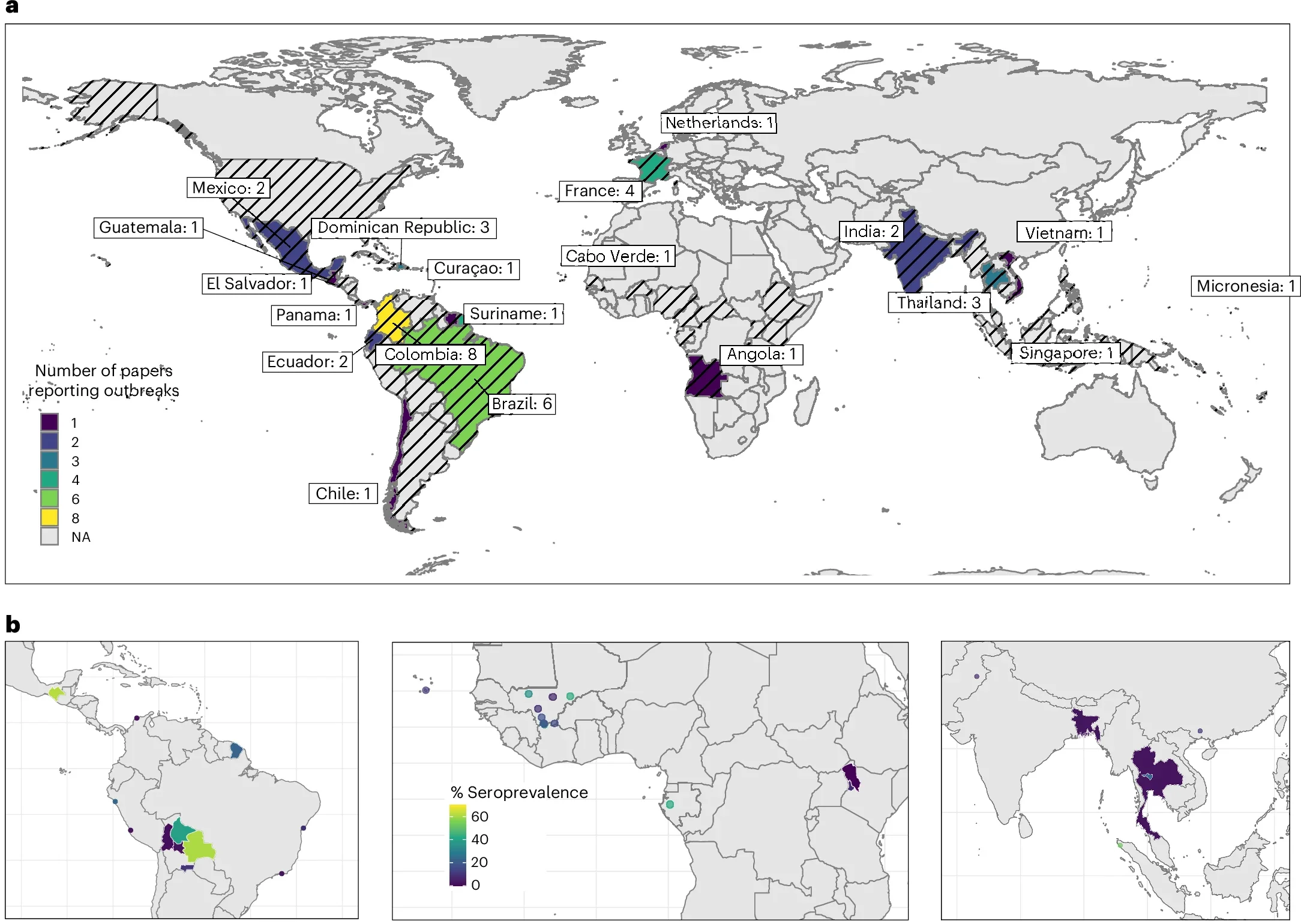
Zika outbreak and seroprevalence mapping. a, Countries with studies reporting ZIKV outbreak information, coloured by number of studies. Outbreaks reported in France and the Netherlands reflect outbreaks in overseas regions. Countries with black diagonal stripes indicate locations where ZIKV transmission has been reported by the WHO78. b, Geolocated areas or regions with ZIKV seroprevalence studies (using IgG assay, HAI/HI, MIA, NS1 BOB ELISA, IFA, capture ELISA and neutralization assays) conducted in the general population in the Americas (left), Africa (middle) and Asia (right). Each dot represents a location-specific estimate, while shaded areas indicate estimates at the administrative-unit level (region, province, district or entire country). Base maps adapted from GADM79. NA, not applicable.
Congenital Zika syndrome occurred in 4.65% of pregnancies with confirmed ZIKV infection (95% CI 3.38–6.67%); pregnancy loss in 2.48%; just over half of infections (51.2%) were symptomatic. Basic reproduction numbers ranged from 1.1 to 7.4. The full database — including all delays, seroprevalence estimates and model parameters — is openly available in the R package epireview (v1.4.5).
The review highlights substantial heterogeneity and inconsistencies in how Zika epidemiological parameters are reported and makes the case for standardised definitions ahead of the next emergence event.