DeZi Webinar: The Nicaragua Cohort
In Part 1 of the DeZi webinar "Cohort & Community Engagement" organised by Wellcome Trust, Eva Harris (UC Berkeley) presents three decades of arbovirus research in Nicaragua and the long-running Pediatric Dengue Cohort Study (PDCS) that anchors much of the field's understanding of dengue immunity, severity, and dengue–Zika interactions.
Harris opens with a timeline running from the late-1990s hospital and health-centre studies through school-based pediatric surveillance (2001–2003), the launch of the community-based PDCS in 2004, evidence-based dengue control interventions, national serosurveys and clinical studies of dengue, chikungunya and Zika, the Zika-era pregnancy cohorts (ZIP, ZPO, NZP) and CARE Groups, and the current CREID urban–rural comparison cohorts and Dengue/ZikaChat intervention studies. A central point of pride: study personnel — over 200 people — are 100% Nicaraguan, and authentic community engagement at every level has been essential to building the trust that turns research subjects into research partners.
Webinar Prof. Eva Harris (UC Berkeley).
The Pediatric Dengue Cohort Study itself is a landmark longitudinal investigation following roughly 4,000 children aged 2–17 each year (originally 2–9, extended stepwise upward), with annual healthy samples plus acute and convalescent sampling around symptomatic episodes. To date, the cohort has enrolled around 11,800 participants and generated more than 140,000 antibody titrations, alongside expansion to chikungunya, Zika and influenza surveillance. A complementary hospital-based study (PDHS) captures the severe end of the clinical spectrum, so together the two platforms span the full arc from inapparent infection to severe disease. Case detection combines RT-PCR/virus isolation, inhibition ELISA and IgM-capture ELISA, and a parallel data-harmonisation pipeline reconciles variables across sites into a master schema for joint analysis.
Harris then walks through the operational backbone that makes a study of this scale possible. The Health Center Sócrates Flores Vivas (HCSFV) provides free 24/7 primary care to all participants, 365 days a year, with standardised protocols and over 150 clinical variables captured per visit. Participants are identified through barcoded ID cards and fingerprint scanning. The annual survey is organised into seven stations — registration, identification, informed consent, anthropometry, structured surveys, blood sampling with CBC, and a non-monetary study gift — while annual field visits use GPS-located households, two-person teams with handheld devices, and tablet-based participation tracking. A custom mobile and web-based capture system, developed by the SSI Nicaragua team itself, has replaced the earlier paper-based workflow. The lab side mirrors this: barcoded sample aliquots and cryogenic labels, automated assay capture (multiplex RT-PCR, IgM-capture and inhibition ELISAs, FRNT validation rules), an OpenClinica-based clinical data platform compliant with Good Clinical Practice, double data entry, audit trails, and a real-time dashboard that flags discrepancies and maps pending samples for field redeployment. An enhanced passive surveillance system reports 94% self-report compliance, 95% presentation within the first 72 hours of fever, and 95% convalescent follow-up, while a three-component consent structure (study participation, long-term sample storage, and genetic studies) is managed with colour-coded paper, barcoding and secure storage.
Cohort participation has grown to nearly 11,800 cumulative participants, with a median 5% annual loss to follow-up (95% retention) and a median participation length of 7 years. Annual satisfaction surveys consistently show the great majority of families rating their experience as "really good" or "excellent."
The scientific impact is substantial. The cohort represents the longest continuous arbovirus cohort in the world. It has driven paradigm-shifting findings on immune correlates of dengue protection and risk, the first demonstration of antibody-dependent enhancement in humans, the role of infection number, sequence and order in DENV–ZIKV interactions (with the striking asymmetry that prior DENV followed by ZIKV does not increase dengue risk, whereas prior ZIKV followed by DENV does — particularly for DENV2), documentation of homotypic re-infections, and a shift in emphasis from antibody quantity to antibody quality (avidity, Fc effector function, neutralising potency).
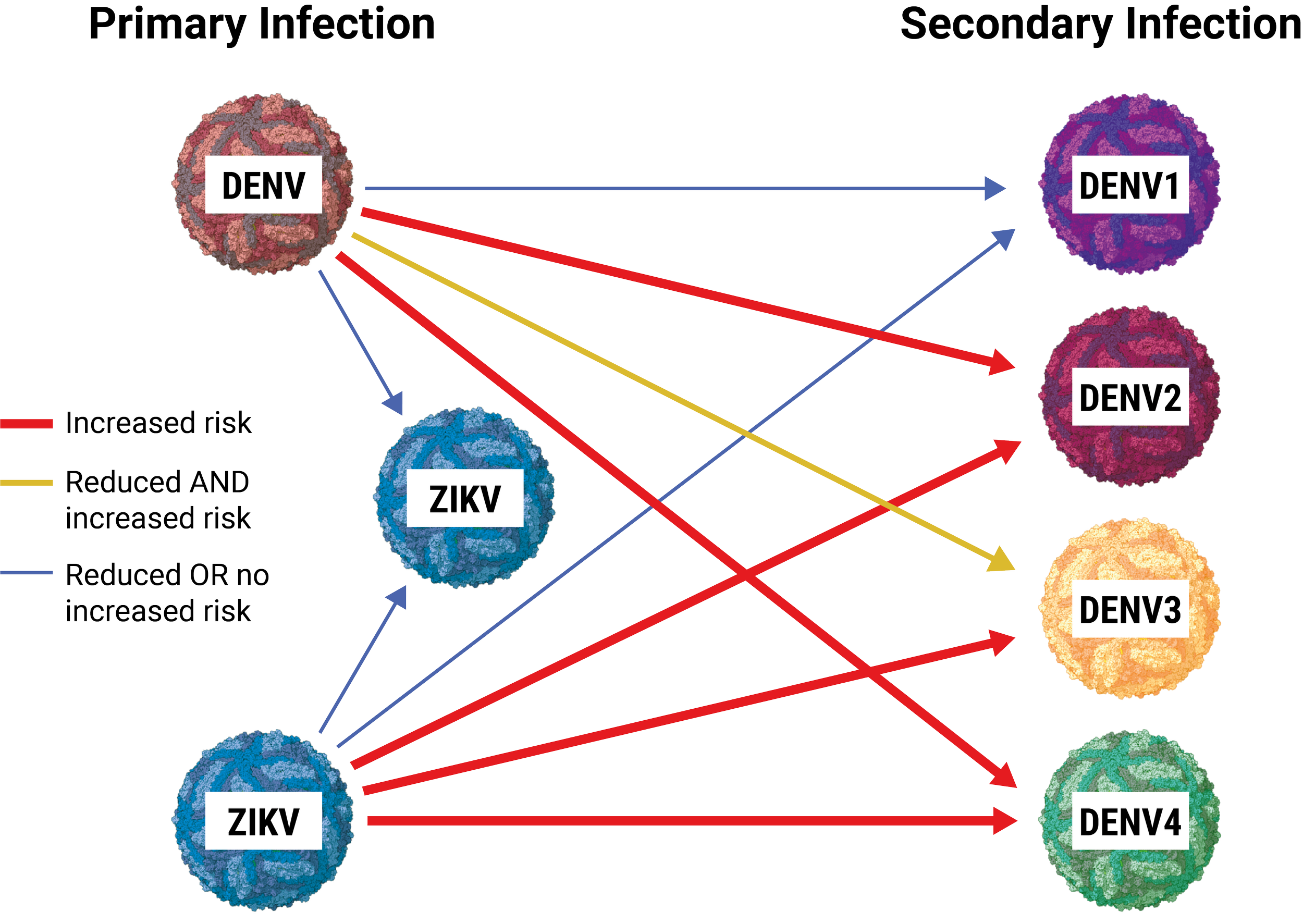
Figure 1. Summary of cross-reactive interactions between prior dengue virus (DENV) and Zika virus (ZIKV) infection and subsequent disease risk. A primary DENV infection reduces the risk of symptomatic DENV1 and ZIKV but increases the risk of severe DENV2 and DENV4 (with mixed effects on DENV3). A primary ZIKV infection reduces the risk of subsequent ZIKV but increases the risk of symptomatic/severe DENV2 and DENV4, shows no increased risk for DENV3, and increases risk for DENV1 — illustrating that pre-existing flavivirus immunity can be either protective or disease-enhancing depending on the serotype/virus combination. Adapted from Katzelnick, L. C., et al. (2020). Current Opinion in Virology; Katzelnick, L. C., et al. (2020). Science. Zambrana, J. V., et al. (2024). Science Translational Medicine.
The body of work has informed the CDC, FDA, WHO, PAHO and ACIP guidance and shapes current dengue and Zika vaccine strategy. Underpinning all of it, Harris argues, is local ownership and autonomy: a bottom-up capacity-building model — onboarding training, continuing education, on-site workshops, in-country MPHs, US-based funded PhDs, and a research governance structure built around an Executive Committee and specialised Technical Committees — that has produced more than 150 peer-reviewed publications, every one of them with Nicaraguan authors, and an in-country research and public-health infrastructure that will outlast any single grant.