Hidden serotype patterns in primary dengue infections
Abstract
Dengue is the most prevalent mosquito-borne viral disease worldwide, yet most primary infections with the four dengue virus serotypes (DENV1–4) cause no symptoms — and what those silent infections look like, by serotype, has remained unknown. Here we leverage 17 years of prospective sample collection from the Nicaraguan Pediatric Dengue Cohort Study (2004–2022) and apply a newly evaluated envelope-domain-III multiplex microsphere-based assay (EDIII-MMBA) to serotype primary inapparent infections at scale. Of 1,626 primary infections detected in 5,931 dengue-naive participants, 77% were inapparent. Serotyping revealed strikingly distinct epidemiological profiles: while symptomatic cases were typically dominated by a single serotype each year, inapparent infections showed a far more complex landscape, with co-circulation of multiple serotypes — including serotypes entirely undetected by symptom-based surveillance for years at a time. DENV3 emerged as the most clinically aggressive serotype, with primary infections more than twice as likely to be symptomatic (OR 2.13, 95% CI 1.28–3.56) and nearly seven times more likely to be severe (OR 6.75, 95% CI 2.01–22.62) than DENV1, while DENV2 had the highest rate of inapparent primary infection. Our findings show that case-based surveillance systematically distorts the epidemiological footprint of DENV and underscore the need for vaccines with balanced immunogenicity across all four serotypes.
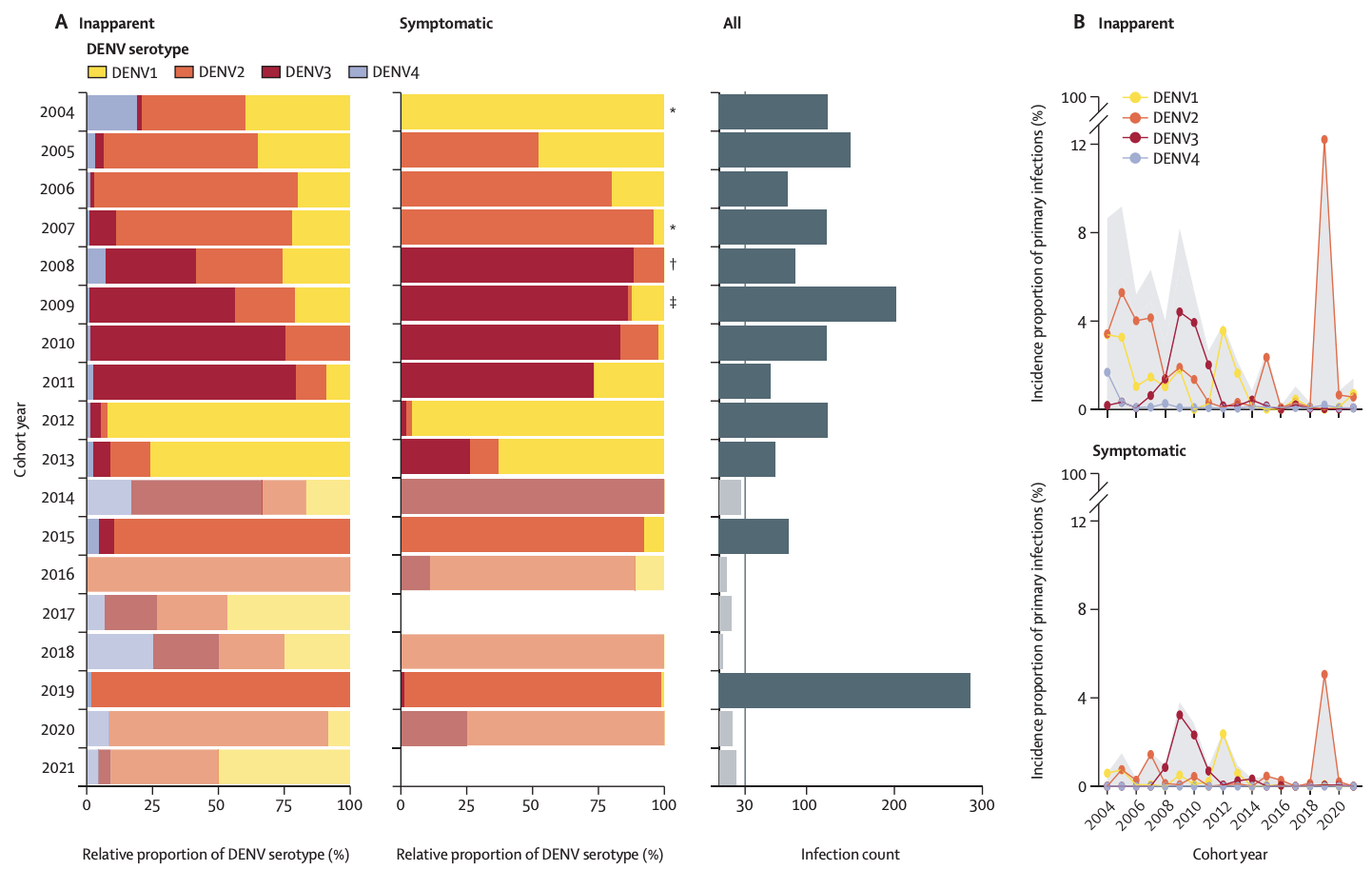
Figure. Serotype distribution in primary symptomatic and inapparent DENV infections in the Pediatric Dengue Cohort Study, 2004–2022. a, Pooled relative distribution of DENV1–4 in inapparent (left) and symptomatic (middle) primary infections by cohort year, with total infection counts (right). Yearly comparisons reveal substantial discrepancies between symptomatic and inapparent fractions: in multiple years (e.g. 2004, 2007, 2008, 2009 — marked *, †, ‡), serotypes circulating silently in the inapparent fraction are entirely absent from symptomatic surveillance. Transparency indicates years with fewer than 30 infections. b, Temporal dynamics of incidence by serotype for inapparent (top) and symptomatic (bottom) primary infections, showing dynamic shifts in serotype dominance — DENV2 in the early years, DENV3 around 2008–10, DENV1 around 2012, and a striking DENV2 resurgence in 2019 reaching 12% of the susceptible population. © 2025, Bos, Zambrana et al., CC BY 4.0.
Behind the paper
This study builds on nearly two decades of partnership between UC Berkeley, the Sustainable Sciences Institute, the Nicaraguan Ministry of Health, and the Sócrates Flores Vivas Health Center in Managua. The Pediatric Dengue Cohort Study has followed roughly 4,000 children every year since 2004, with annual healthy-sample collection that allows us to detect the silent infections that conventional case surveillance never sees.
The key methodological breakthrough was scaling up an envelope-domain-III multiplex microsphere-based assay (EDIII-MMBA) to serotype primary infections directly. Gold-standard neutralisation assays are slow, sample-hungry, and impractical for analysing thousands of samples — which is why the global dengue field has remained largely blind to serotype patterns in inapparent infection. The EDIII-MMBA showed 100% sensitivity, specificity, and accuracy against both RT-PCR and FRNT, and works without Biosafety Level 2 infrastructure or live virus.
Pairing this tool with 17 years of cohort samples revealed something we did not expect: the dengue you see in the clinic is fundamentally a different epidemic from the dengue actually circulating. Symptomatic cases give a tidy picture of one dominant serotype per year; inapparent infections reveal hidden co-circulation, including years when a "missing" serotype was quietly transmitting throughout the community. The serotype-level differences in disease spectrum — particularly DENV3's striking symptomatic and severe profile, even in primary infections — reframe how we should think about vaccine design and the populations at risk.
Context
International collaborations and long-term cohort infrastructure underpin our ability to read the silent half of the dengue epidemic. By coupling high-throughput serotyping with prospective community surveillance and statistical modelling, we move from descriptive snapshots to a real-time understanding of how each DENV serotype contributes to disease burden — work that is now being extended to other endemic settings to test whether DENV3's aggressive profile is a global pattern or a regional one.